REMEMBERING FABIAN: A YATS TUITION ASSISTANCE
Personal Data Sheet
STUDENT’S NAME__________________________________________ AGE___________
DATE OF BIRTH________________ GRADE ENTERING IN FALL___________
SCHOOL_________________________________________________________________
PARENT’S /GUARDIAN’S NAME____________________________________________________________________
ADDRESS__________________________________CITY_______________ZIP____________
PHONE____________________________CELL______________________________________
PARENT’S EMAIL____________________________________________________________
NUMBER OF ADULTS IN HOUSEHOLD_________
NUMBER OF CHILDREN UNDER 21 IN HOUSEHOLD___________
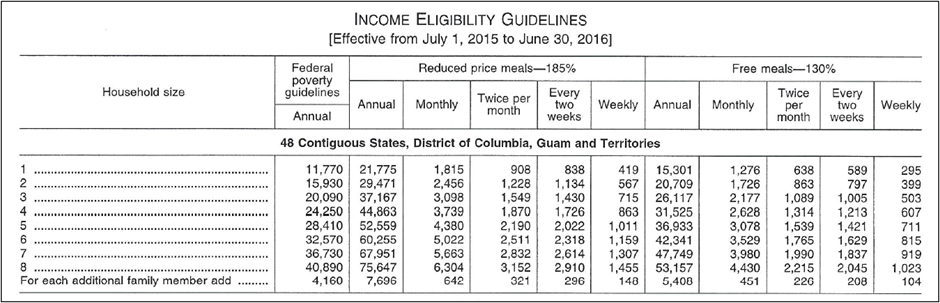
IS THE STUDENT ELIGIBLE FOR FREE OR REDUCED LUNCH?
YES________ NO_______
IF YES, PLEASE INDICATE
FREE LUNCH___________ OR REDUCED LUNCH___________
REASON FOR REQUESTING TUITION ASSISTANCE ______________________________
______________________________________________________________________________
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
STUDENT’S NAME_____________________________________________
THIS IS A NEED-BASED TUITION ASSISTANCE. PLEASE INDICATE YOUR YEARLY INCOME. (If needed, use the chart below.)_________________________________
Please return the COMPLETED APPLICATION to include this PERSONAL DATA SHEET, along with the following attachments to the address listed below.
- The student (age 8 years and above) must write and submit a SENTENCE OR PARAGRAPH stating why he/she wants to participate in the YATS Summer Program. (Although previous experience on stage is not required, the student may include information about his/her experience/interest in the areas of dance, music, or theatre).
- A LETTER OF RECOMMENDATION from an adult who knows the student from his/her current school, community activities, or faith-based programs.
***BE SURE THE STUDENT’S NAME IS WRITTEN AT THE TOP OF EACH PAGE BEING SUBMITTED.
SEND COMPLETE APPLICATION PACKAGE TO:
REMEMBERING FABIAN
PO BOX 969
SLIDELL, LA 70459